
Presenting Reason
66 year old Caucasian female, came into clinic today for a visual field disturbance, went to to Sydney Eye Hospital and said she was suspect GCA but no evidence on MRI or blood tests. Upon examination, normal anterior segment and early cataracts found, ceased plaquenil 200mg 3/12 ago after taking it for 10 years. nil changes in central vision, nil pain, nil current flashes/floaters, nil diplopia. No episodes since then.
Medical History
- Nil Allergies
- Nil previous eye surgery, trauma or orthoptic management
- Unremarkable family history
- Rheumatoid Arthritis
- Current Medication: Methotrexate 20mg, Xeljanz, Multivitamins
Clinical Exam
- Vision c gls
R 6/6 (N5) L 6/6 (N5) - Glasses Prescription
R +1.00DS / 0.00DC x 180 (Add +2.25DS)
L +0.75DS / +0.25DC x 28 (Add +2.25DS) - IOP c Goldmann Applanation
R 18mmHg L 18mmHg - Nil RAPD
- Angles Open
Clinical Tests
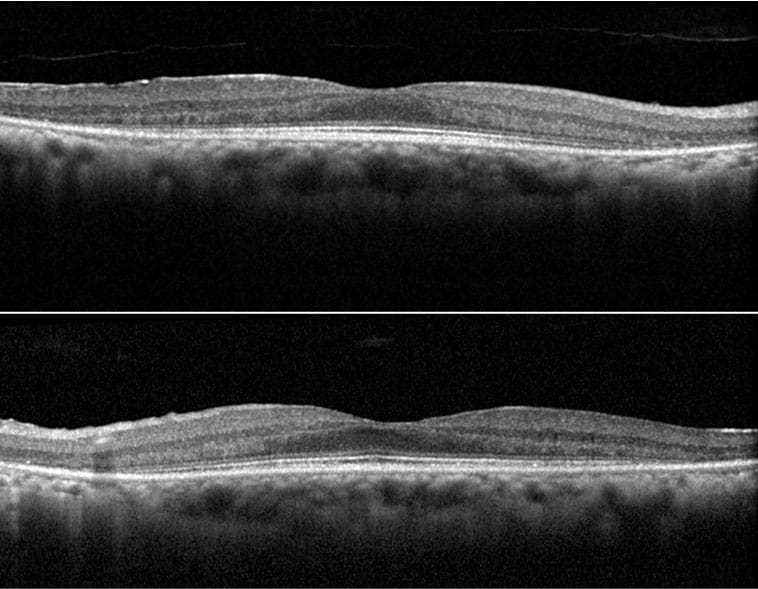
Macular scan
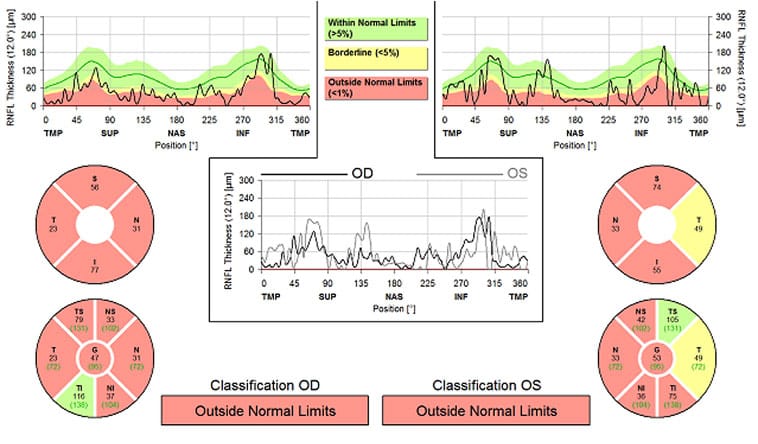
Optic Nerve (RFNL scan)
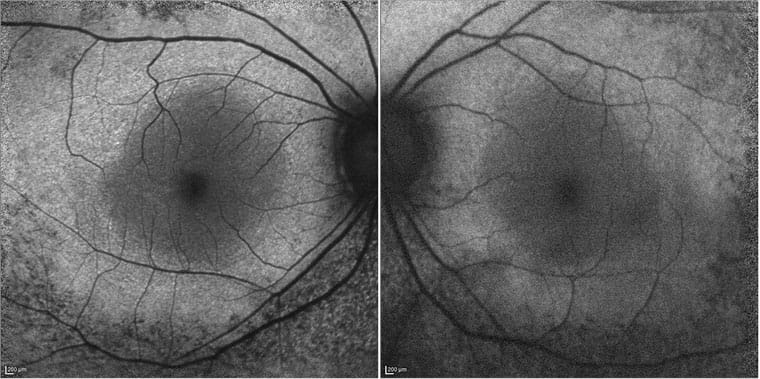
Fundus Autofluorescence
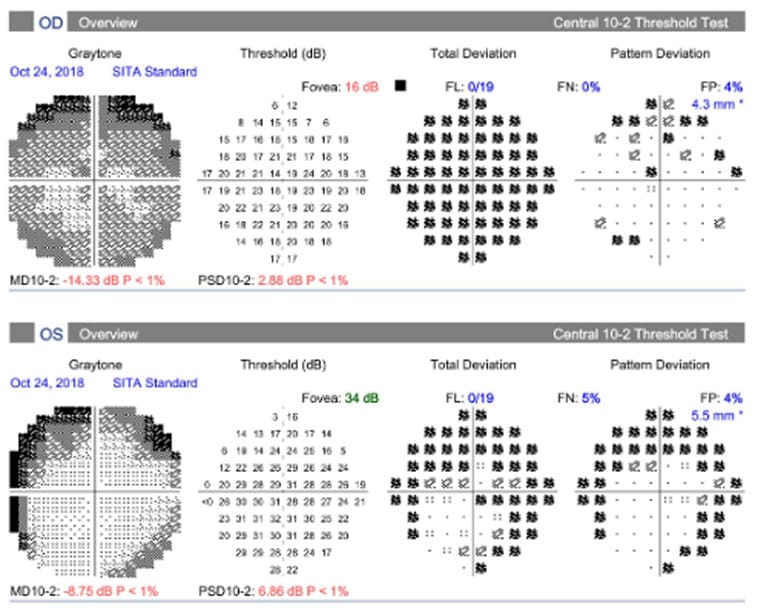
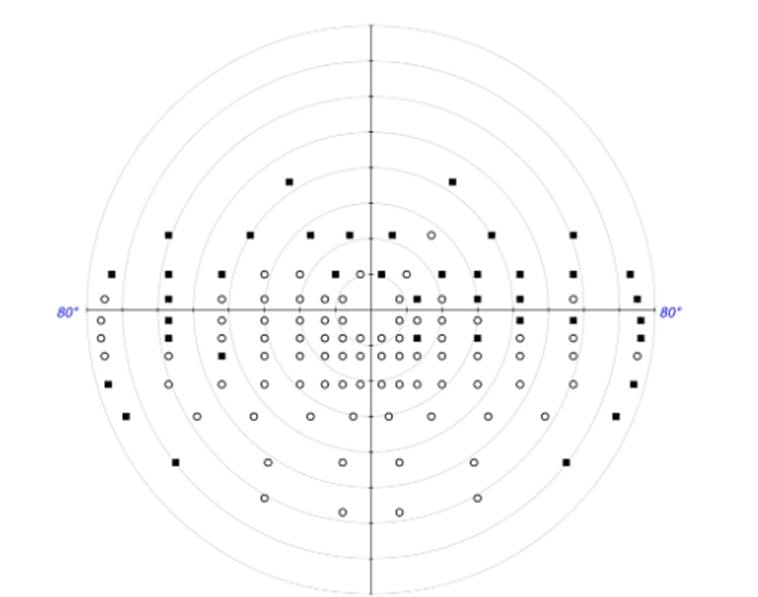
Visual Field (HVF10-2 + Binocular Estermann)
Binocular Estermann
Diagnosis
Treating Ophthalmologist for this case: Dr Helene Cass
Plaquenil Retinal Toxicity
Upon further questioning, patient has been diagnosed with plaquenil toxicity at another eye clinic, but continued to do her normal things in life until her episode of flashing lights. Visual Field testing shows reduction in sensitivity outside the central 10 degrees in both eyes, this pattern of toxicity commonly seen in people of Asian descent. Binocular Estermann not too good and advised to not drive at night or low light. Discussed that last visual field not sufficient for Conditional Licence and would need to do further assessments if patient very much wanted to keep driving, no guarantee. Patient has been coming back every 6 months and upon examination, central acuity remains good at 6/6 both eyes, with early cataracts, but peripheral vision remains poor.
What is plaquenil toxicity?
Plaquenil (aka Hydroxychloroquine) is a medication used for various rheumatologic and dermatologic conditions. Prolonged use of this drug can cause it to effect ocular structures such as the cornea, ciliary body and the retina, but symptoms vary person to person. Risk factors include people with renal impairment, concomitant Tamoxifen use and pre-existing retinal issues.
Signs and Symptoms?
Patients with early stages of toxicity are often asymptomatic to any visual changes. Retinal changes can be detected by high quality OCT scans and visual field tests, supplemented by a detailed anterior segment and fundus exams by an ophthalmologist. Often people with late stage toxicity complain of visual color deficits, specifically red objects, missing central vision, difficulty reading, reduced or blurred vision, glare, flashing lights, and metamorphopsia.
Prognosis?
Unfortunately, even after the cessation of the drug the retinopathy that ensues is not reversible. The earlier the toxicity is recognized, the greater the chance of visual preservation. RANZCO guidelines suggest baseline exam in first year of drug use and annual screening after 5 years of use for patients with no risk factors. Examination should always include OCT + autofluorescence, Visual Field testing, and dilated fundus exam.