
Presenting Reason
72 year old Caucasian female, came into clinic today for an urgent review. Patient complaining of seeing a grey line and patterns in visual field for the past 3 days. Feeling slightly nauseous, nil headache. GP concerned of possible stroke.
Medical History
- Nil Allergies
- Left Amblyopia
- Hypertension, GORD, Stents in heart
- Unremarkable family history
- Current Medication: Atorvastatin, Ativan, Citalopram, Micardis, Rabeprazole, Aspirin, Nitrolingual Spray, Deptran, Ducolax
Clinical Exam
- Vision c gls
R 6/12 (N8) L 6/36 (N18) - Glasses Prescription
R +0.00DS / +0.50DC x 10 (Add +3.00DS)
L +1.00DS / +0.25DC x 28 (Add +3.00DS) - IOP c Goldmann Applanation
R 12mmHg L 14mmHg - Nil RAPD
- Angles Open
- Ishihara R + L NAD
Clinical Tests
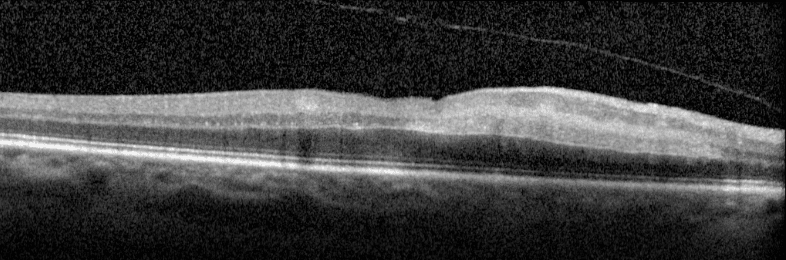
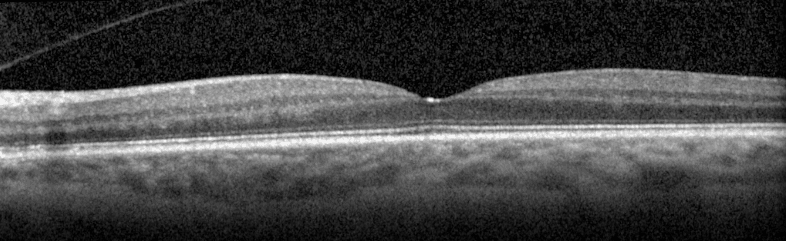
Macular Scan
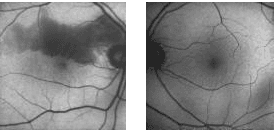
Fundus Autofluorescence
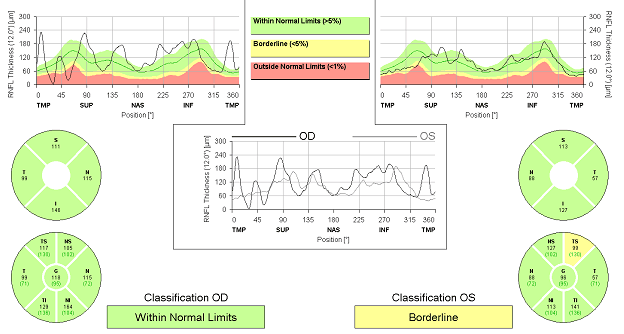
Optic Nerve (RFNL scan)
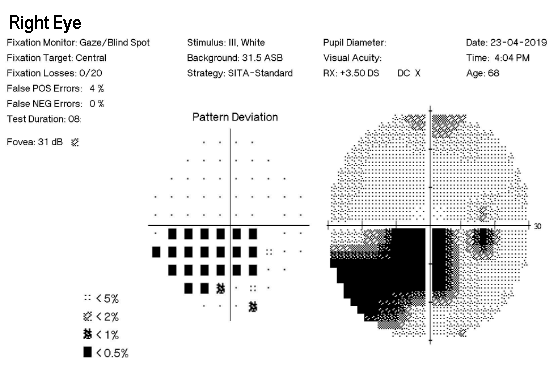
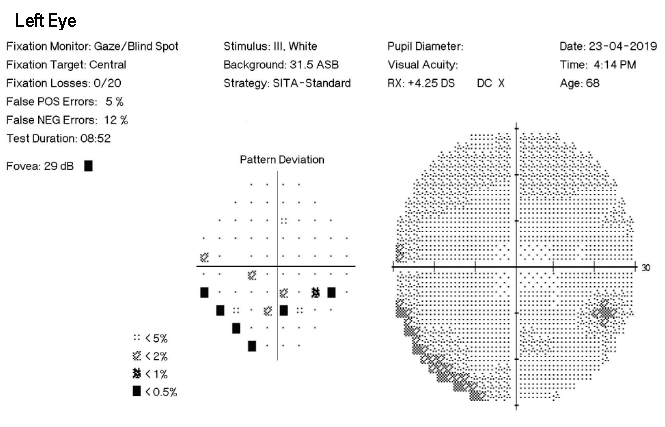
Visual Field (HVF30-2)
Diagnosis:
Treating Ophthalmologist for this case: Dr Terence Tan
Branch Retinal Artery Occlusion (BRAO)
Retinal Imaging confirmed the oedema on the right inferior macula and retinal pallor was consistent with a right superior branch artery occlusion. We sent the patient away to get a carotid ultrasound (which showed minimal stenosis), echocardiogram, and ECG. Subsequent visit did not show any neovascularization of the affected area and Binocular Estermann qualified patient to meet driving requirements. We encouraged the patient to routinely return to the practice to have their visual fields and OCT scans monitored for neovascularization and driving eligibility.
What is a BRAO?
A retinal artery occlusion is classified as an ophthalmic emergency as there is an obstruction to the blood flow as a result of a possible clot. Patients sometimes can have a concurrent stroke which is why we need to get a quick diagnosis and send them off to detect any emboli causing the obstruction. The lack of blood and oxygen that is delivered to the eye can cause sever vision loss if not picked up promptly. In this case the embolism was blocking the supply to the branch retinal artery, but occlusions can occur in the cilioretinal, central, and ophthalmic artery. Common risk factors for patients who retinal artery occlusions include old age, smoker, high blood pressure, high cholesterol, obesity, diabetes, coagulopathy.
Signs and Symptoms?
Patients may often complain of sudden, painless loss of vision in one or both eyes. Complete loss of vision may indicate a blockage further back near the ophthalmic artery, and visual defects are often associated with branch artery occlusions. 6/6 vision with these symptoms can indicate an occlusion of the cilioretinal artery which can be confirmed with dilated fundus exam. Patients must always be screened for a concurrent Giant Cell Arteritis as other signs may include headache, RAPD in the affected eye and a cherry red spot over the fovea in colour photos.
Prognosis?
The recovery is very slow in these situations and depends on the level of oedema that was occurred during the stroke. Some patients may develop a neovascularization of the retina which can be treated with anti-VEGF injections. These patients are also at a risk of developing secondary glaucoma from iris neovascularization. Examination should always include OCT + auto fluorescence, Visual Field testing, and dilated fundus exam.